AI-powered rostering, built for emergency medicine.
Built for emergency medicine. AI rostering for ED-like teams.
IRIS was designed where rostering is hardest — ED, ICU, anaesthetics and paramedics — then scaled hospital-wide. Explainable AI, fairness audits, SSO, audit logs and regional hosting support acute services without turning rosters into a black box.
Evaluating for your department? Start a trial · Contact us

15×
faster runs
3.0
IRIS narration
5
roster levels
Most roster platforms are adapted for emergency medicine. Intelligent Roster was built from it.
Built where rostering is hardest. Calm enough for daily use. Structured for the whole health service — and the ED-like teams beyond it.
Adaptive roster intelligence
IRIS gets sharper the more your team uses it.
The roster intelligence that improves at the pace your service actually changes — grounded in your structure, your rules, and every decision you review.
Learns from your service model
Streams, scopes, fatigue rules, and fairness settings shape every suggestion. IRIS works inside your configured structure — not a generic template.
Two model pathways, one workflow
Claude for deep roster reasoning. GPT for fast lookups and summaries. Each used where it helps most.
See AI Tech →IRIS 3.0 narrates and explains
Live progress during Generate and Fill Gaps, end-of-session summaries with fill rates and rejection reasons, and honest diagnostics when slots stay empty.
See latest release notes →Human review stays in control
Every roster is reviewed before publishing. Every suggestion comes with a reason. IRIS assists; your team decides.
Privacy Act and APPs
Designed around Australian privacy expectations and GDPR where applicable.
Full audit logging
Roster actions, approvals, and overrides are recorded for review and governance.
Workforce data only
No patient data stored or processed. Ever.
Enterprise SSO & MFA
Microsoft, Google, OIDC, and native MFA supported.
For roster builders
ED-like rostering is genuinely hard. That is not a failure on your part.
Variable demand, senior cover, fatigue rules, leave pressure, and fairness — all at once. Intelligent Roster was shaped around that reality in emergency medicine, and carries the same discipline into every ED-like team.
Demand does not arrive evenly
Emergency and acute services change by hour, day, stream, and season. A useful roster has to understand that shape before shifts are assigned.
Fairness is operational
Nights, weekends, unpopular shifts, senior cover, and leave pressure need evidence over time, not memory or negotiation.
Safety rules need structure
Fatigue, rest periods, scope of practice, contracted hours, and approved leave must be visible before publication and after changes.
Governance needs a record
Workforce leaders need data boundaries, audit logs, regional hosting choices, and documented reasons for roster decisions.
Your best results come in ED-like environments
Because Intelligent Roster was built for emergency medicine, it fits teams that roster like ED: 24/7, safety-critical, rule-heavy, and politically sensitive around fairness and fatigue.
24/7 operations
Extended hours, overnight cover, and demand that does not follow a nine-to-five pattern.
Safety-critical
Fatigue risk, scope of practice, senior cover, and rest rules that cannot be negotiated away.
Rule-heavy
Awards, contracted hours, qualifications, and local policy encoded before anyone is assigned.
Fairness & fatigue politics
Weekends, nights, leave pressure, and unpopular shifts need evidence — not memory or corridor deals.
Healthcare today
Start with other hospital services. Expand across acute care.
These are closest to what we built for ED — so the product fits almost immediately, and whole-service deals become natural, not forced.
Acute hospital services
Same complexity as ED: fatigue rules, senior cover, skill mix, training needs, leave pressure, and fairness.
Allied & diagnostic services
Extended hours or 24/7 operations with on-call patterns, variable demand, and coverage gaps to manage.
Virtual & community acute
Strong shift patterns, lots of part-timers, and high need for fairness and flexibility across distributed teams.
Ambulance & transport
Fatigue risk, scope of practice, and rapid short-notice change — the same operational pressure as acute care.
Aged care & disability
Big 24/7 workforce, chronic staffing gaps, weak legacy tools, and increasing regulatory scrutiny.
Mental health & behavioural care
High-acuity staffing, continuity needs, skill mix, safety constraints, and last-minute demand changes.
Broader horizons
The same architecture fits beyond healthcare
Any team that rosters like ED — 24/7, safety-critical, rule-heavy, and sensitive around fairness — shares the operational DNA Intelligent Roster was built for.
Call centres & contact centres
Demand curves across the day, coverage pressure, fairness tracking, and shrinkage — the same rostering logic in a different uniform.
Transport & aviation
24/7 safety and fatigue rules, union agreements, and complex shift patterns that generic tools struggle to hold together.
Police, fire & emergency services
Unpredictable workload, public safety limits, legal constraints, and fairness politics that mirror acute-care rostering.
Security & facilities
Multi-site coverage, variable demand, and teams that need the same governed swap, leave, and fairness workflows.
See IRIS in action
A guided walkthrough of how Intelligent Roster® and IRIS work in real clinical environments.
Built for the hardest rostering environment first
Emergency-first structure
Streams, scopes, senior cover, and demand patterns are modelled before anyone is assigned.
A living roster, not a spreadsheet
Availability, leave, swaps, gaps, and short-notice changes stay connected as the roster moves.
Explainable by design
Every suggestion has context. Every exception can be reviewed. People remain accountable.
I used to build rosters in Excel
I started with a spreadsheet because that is what everyone did. One grid became two, then three, and before long I was managing versions, emails, and exceptions across multiple files. On paper the roster looked reasonable, but in reality it was both over-rostered and under-utilised at the same time.
The whole roster, connected
The platform starts with ED complexity, then carries the same discipline into hospital-wide services, ambulance, aged care, and other ED-like teams.
IRIS helps build the roster
Generate, fill gaps, or validate the roster with reasons surfaced before publishing.
Swaps stay governed
Direct, open, or pickup shifts can move quickly while hard safety rules and approvals remain visible.
Leave is part of the roster
Requests, balances, conflicts, and downstream coverage impact are visible before approval.
Fairness can be explained
Weekends, nights, hours, preferences, and unpopular shifts are tracked over time.
Acute changes are expected
Sick calls, demand shifts, and coverage gaps can be handled without losing the roster picture.
Built for ED-like teams
SSO, MFA, audit logs, role-based access, and regional hosting — from ED to whole health services and beyond.
The Five Levels
Structure first, then shifts. The better Levels 1–4 are set up, the better every IRIS suggestion.
| Level | Purpose | Your Role |
|---|---|---|
| 1 Streams & Shift Patterns | Which shifts can exist — by department and shift type (AM, PM, Night, Long Day). | Define your streams and the shift patterns that belong to each one. |
| 2 Vacancy Planning | How many staff are needed per shift — by craft group, scope, and mandatory skills. | Set required roles and mandatory qualifications per shift and day. |
| 3 Master Roster | Repeatable baseline patterns and core coverage — your sensible starting point. | Maintain templates so IRIS has a reliable foundation for suggestions. |
| 4 Staff Availability | When people can and prefer to work. Set via My Availability. Highest priority input. | Encourage staff to keep availability up to date — it directly improves suggestions. |
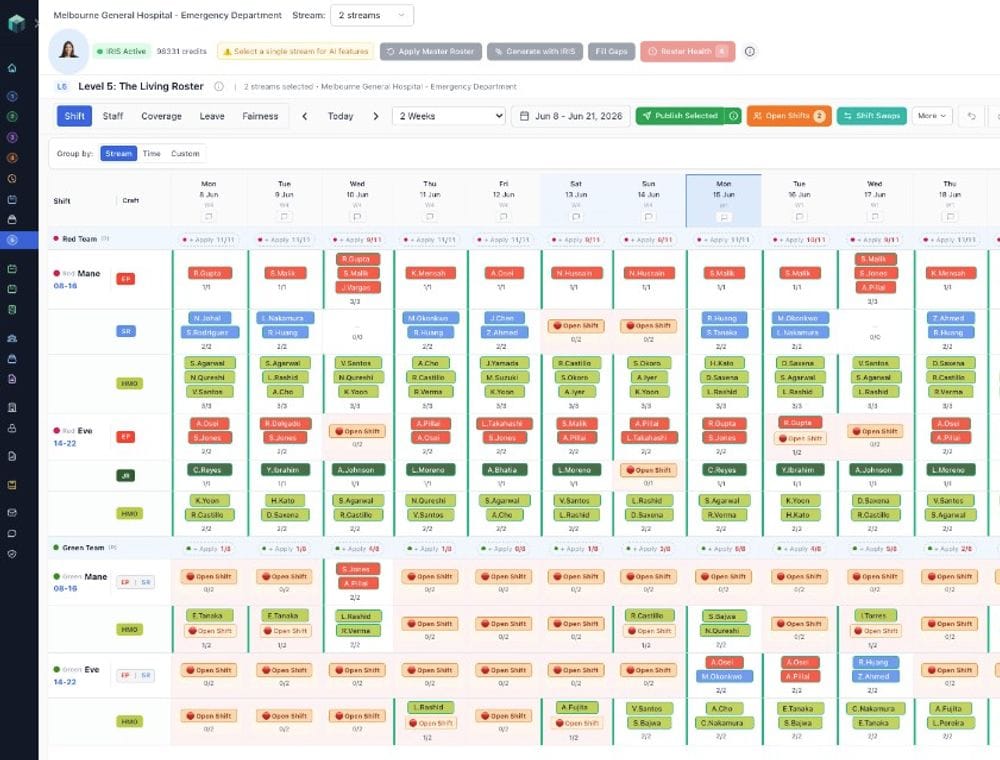
| 5 The Living Roster ✦ | The actual roster: who is assigned to what, when. This is where IRIS works with you. | Use IRIS here to generate, fill gaps, validate, and publish. |
From service structure to living roster
Model the service
Set streams, shift patterns, roles, scopes, demand, and organisational rules.
Build with IRIS
Ask IRIS to generate, fill gaps, or validate the roster against your configured structure.
Review, publish, adapt
Approve with human judgement, then manage leave, swaps, gaps, and changes in the living roster.
Evidence you can inspect.
First ED roster generated
A structured first pass with conflicts, gaps, and reasons visible for review
These examples are framed as operational signals, not promises. Your roster remains reviewed by your team before publication.
Living with IRIS
Real experiences from roster builders, managers, and clinicians.

“Now, when a sick call comes in early in the morning, I am not scrambling. I can see who has availability, who is safe to work, and who is already carrying load. The biggest change has not been speed. It has been control.”
I used to build rosters in Excel
Questions health services ask first
Is Intelligent Roster only for emergency departments?
No. It was built first for emergency medicine because ED rostering is the hardest test: variable demand, senior cover, fatigue risk, scope, leave, and short-notice change. The same structure supports ICU, wards, theatres, ambulance, virtual care, aged care, and other ED-like teams across a whole health service.
Does it work for ambulance, aged care, or hospital-wide rostering?
Yes. Ambulance, retrieval, and NEPT providers share ED-like fatigue and scope pressures. Aged care runs 24/7 with chronic gaps and rising scrutiny. Hospital-wide deals — ICU, allied health, virtual wards — are a natural expansion from an ED-first foundation.
What about call centres, transport, or other non-health sectors?
The same architecture fits any ED-like environment: 24/7, safety-critical, rule-heavy, and sensitive around fairness. Call centres, transport, emergency services, and facilities teams share that operational DNA even when the uniform changes.
Will it respect our organisational rules?
Rules are configured around your service: rest periods, consecutive shifts, scope, leave, contracted hours, and local policy. IRIS works inside that structure and surfaces conflicts for review.
What if IRIS gets it wrong?
IRIS is an assistant, not a black box. You review every roster before publishing. Every suggestion comes with a reason.
Where is our data stored?
You choose at signup: Global (Render, Singapore) or Australian (AWS Sydney). Same security bar, different geography.
Do you store patient data?
No. IRIS holds workforce data only — schedules, availability, leave, and shift information. Technically enforced.
How long until staff can use it?
Staff get the app the same day you publish. Most are comfortable within their first shift.
Built for ED-like teams in healthcare and beyond. Trust Centre
See how an ED-first roster platform works.
From emergency departments to whole health services — and the ED-like teams beyond them.